
INTRODUCTION
While septoplasty is a commonly performed operation in adults, its use in children is less frequent and controversial. Paediatric Septoplasty is performed by a paediatric ENT specialist with unique training and expertise in managing nasal issues in children and teens. The procedure was first described in 1902 by Freer [1], but initial results were unfavourable, leading to deformities such as saddle nose and maxillary retrusion. In the 1950s, surgeons cautioned against performing septoplasty in children, fearing that resection of the quadrilateral cartilage would impair nasal growth [2]. Farrior and Connolly reinforced this belief in the 1970s, arguing that nasal surgery should be delayed until complete nasal development [3]. However, later studies and clinical observations began to support the safety and necessity of paediatric septoplasty in appropriately selected cases [4].
DEBUNKING THE MYTH: DOES PAEDIATRIC SEPTOPLASTY/ SEPTORHINOPLASTY AFFECT GROWTH?
Early concerns about paediatric Septoplasty and Septorhinoplasty were based on flawed animal studies where aggressive septal cartilage removal without mucoperichondrium preservation led to growth inhibition [5]. Research by Hartshorn and others indicated that septal cartilage removal with mucoperichondrial preservation did not impede facial growth, affirming that modern conservative techniques can preserve nasal and maxillary development [6].
Jugo and Triglia et al. conducted human studies in the 1990s, demonstrating that paediatric external septoplasty, when performed appropriately, does not cause adverse anthropometric effects [7]. Additional anthropometric studies confirmed that septoplasty does not significantly alter facial skeletal growth, and Tasca et al. in 2011 validated these findings with long-term follow-up on endonasal paediatric septoplasty cases [8].
UNDERSTANDING NASAL GROWTH CENTRES
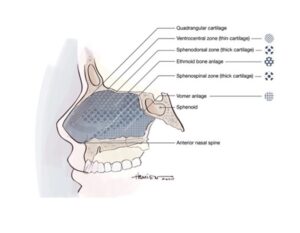
Figure : Original figure by Grant S. Hamilton, III. The neonatal nasal septum showing ventrocentral area of thin cartilage, sphenospinal zone, and sphenodorsal zone.
The nasal septum plays a pivotal role in facial development, particularly in the sphenodorsal and sphenospinal zones [9]. Research highlights that preserving the mucoperichondrium is crucial for maintaining nasal growth [10]. Failure to intervene when necessary can result in progressive nasal obstruction, worsened facial asymmetry, and compromised maxillary growth [11].
INDICATIONS FOR SEPTORHINOPLASTY IN CHILDREN
Paediatric septorhinoplasty is indicated for multiple conditions, including:
- Septal abscess with cartilage necrosis – This is an emergency and requires immediate septal reconstruction.
- Severe Nasal Obstruction – Chronic breathing issues can impair sleep, learning, and exercise tolerance [12].
- Obstructive sleep apnoea.
- Post-Traumatic Deformities – Early correction can prevent long-term functional and aesthetic complications [13].
- Congenital Malformations – Conditions such as dermoid cysts and cleft lip and palate necessitate surgical intervention [14].
- Progressive Nasal Distortion – Delay in correction can lead to worsened asymmetry [15].
- Saddle Nose Deformity – Delayed treatment can lead to nasal contracture, complicating future interventions [16].
THE RISKS OF DELAYING SEPTORHINOPLASTY IN CHILDREN
Delaying necessary surgery in children with nasal deformities can have long-term consequences, including:
- Nasal Contracture and Structural Collapse – Progressive contracture of soft tissues can lead to severe deformities [17].
- Deficient Skin Envelope – Delayed intervention may necessitate complex reconstructive procedures [18].
- Psychosocial Impact – Nasal deformities can contribute to social stigma and self-esteem issues [19].
COMPARING SURGICAL AND NON-SURGICAL MANAGEMENT OPTIONS
While mild cases may be managed with nasal stents, CPAP, or steroid sprays, these options provide only temporary relief [20]. In severe cases, septoplasty is required to restore function and prevent long-term complications [21].
THE CHANGING ANATOMY OF THE NASAL SKELETON
The paediatric nasal skeleton undergoes significant changes during development [22]. The cartilaginous septum reaches its maximum size by age two, with subsequent growth occurring primarily through ossification [23]. Two critical nasal growth periods have been identified: infancy and puberty. Historically, elective septoplasty was delayed until adolescence, but contemporary evidence suggests that early intervention can be beneficial in select cases [24].
THE IMPORTANCE OF SURGICAL TECHNIQUE
Surgical success in paediatric septoplasty depends on:
- Preservation of the Mucoperichondrium – Essential for cartilage regeneration [25].
- Conservative Cartilage Resection – Techniques such as cartilage overlap maintain nasal structure [26].
- Appropriate Timing – Surgery is recommended from age six onward in functionally impaired children [27].
- Minimally Invasive Techniques – Endoscopic approaches reduce trauma and improve recovery [28].
ETHICAL AND PARENTAL CONSIDERATIONS
Paediatric septorhinoplasty involves ethical considerations regarding informed consent and long-term follow-up [29]. Parents should be thoroughly counselled about the benefits and potential risks of surgery.
CONCLUSION
Contemporary research overwhelmingly supports the safety and efficacy of paediatric septoplasty and septorhinoplasty. Studies show that delaying necessary surgery can lead to worsened outcomes, including nasal obstruction, asymmetry, and psychosocial distress. With proper technique and timing, these procedures can restore nasal function, improve aesthetics, and enhance overall quality of life.
Breathe Better, Live Better: Expert Paediatric Septoplasty & Septorhinoplasty in Singapore with Dr Sandeep Uppal
Is your child struggling with persistent nasal blockage, difficulty breathing, or recurrent sinus infections? A deviated nasal septum or structural nasal issues could be the cause.
Dr. Sandeep Uppal, an internationally recognised specialist in Facial Plastic Surgery, Rhinology, and ENT – Head & Neck Surgery, offers expert paediatric Septoplasty and Septorhinoplasty to restore both function and aesthetics. With his extensive experience in rhinoplasty and nasal airway surgery, Dr. Sandeep provides personalized, child-friendly care to ensure the best possible outcomes for your little one.
Why Choose Dr. Sandeep Uppal?
✅ Dual Expertise in ENT & Facial Plastic Surgery – Ensuring both functional improvement and natural aesthetics
✅ Specialized Approach for Paediatric Cases – Gentle techniques tailored for growing facial structures
✅ Comprehensive Care – Addressing nasal breathing issues, sinus health, and facial harmony
✅ Trusted Internationally – Board-certified and a leader in the field of facial plastic surgery
Give your child the gift of easy breathing and confidence. Schedule a consultation with Dr. Sandeep Uppal today!
REFERENCES
- Freer O. The Correction Of Deflections Of The Nasal Septum With A Minimum Of Traumatism. JAMA. 1902;XXXVIII(10):636.
- Grymer L, Bosch C. The nasal septum and the development of the midface. Rhinology. 1997;35(1):6-10.
- Gilbert J, Segal S. Growth of the Nose and the Septorhinoplasty Problem in Youth. Plast Reconstr Surg. 1959;23(3):293.
- Farrior RT, Connolly ME. Septorhinoplasty in Children. Otolaryngol Clin North Am 1970;3:345-64.
- Sarnat B, Wexler M. The Snout After Resection of Nasal Septum in Adult Rabbits. Arch Otolaryngol. 1967;86(4):463-466.
- Hartshorn DF. Facial Growth Effects of Nasal Septal Cartilage Resection in Beagle Pups. Iowa City, IA: University of Iowa Press; 1970.
- Bernstein L. Early submucous resection of nasal septal cartilage: a pilot study in canine pups. Arch Otolaryngol. 1973;97(3):273-278.
- Cupero T, Middleton C, Silva A. Effects of Functional Septoplasty on the Facial Growth of Ferrets. Arch Otolaryngol. 2001;127(11):1367.
- Triglia JM, Cannoni M, Pech A. Septorhinoplasty in children: Benefits of the external approach. J Otolaryngol 19:274-278, 1990.
- Jugo S. Total Septal Reconstruction Through Decortication (External) Approach in Children. Arch Otolaryngol. 1987;113(2):173-178.
- Bejar I, Farkas LG, Messner AH, and Crysdale WS. Nasal growth after external septoplasty in children. Arch Otolaryngol Head Neck Surg 122:816-821, 1996.
- El-Hakim H, Crysdale W, Abdollel M, Farkas L. A Study of Anthropometric Measures Before and After External Septoplasty in Children. Arch Otolaryngol. 2001;127(11):1362.
- Walker PJ, Crysdale WS, and Farkas LG. External Septorhinoplasty in children: Outcome and effect on growth of septal excision and reimplantation. Arch Otolaryngol Head Neck Surg 119:984–989, 1993.
- Tasca I, and Compadretti GC. Nasal growth after paediatric septoplasty at long-term follow-up. Am J Rhinol Allergy 25:e7–e12, 2011.
- Tatum S. Paediatric Facial And Reconstructive Surgery, An Issue Of Facial Plastic Surgery Clinics Of North America, E-Book.; 2014:503-508.
- Vetter U, Pirsig W, Helbing G, et al. Patterns of growth in human septal cartilage: A review of new approaches. Int J Pediatr Otorhinolaryngol 7:63–74, 1984.
- Verwoerd C, Verwoerd-Verhoef H. Rhinosurgery in Children: Basic Concepts. Facial Plastic Surgery. 2007;23(4):219-230.
- Kawalski H, Śpiewak P. How septum deformations in newborns occur. Int J Pediatr Otorhinolaryngol. 1998;44(1):23-30.
- Christophel JJ, and Gross CW. Paediatric septoplasty. Otolaryngol Clin North Am 42:287–294, ix, 2009.
- Alshaikh N, Lo S. Nasal septal abscess in children: From diagnosis to management and prevention. Int J Pediatr Otorhinolaryngol. 2011;75(6):737-744.
- D’Ascanio L, Lancione C, Pompa G, et al. Craniofacial growth in children with nasal septum deviation: A cephalometric comparative study. Int J Pediatr Otorhinolaryngol 74:1180–1183, 2010.
- Blahova O. Late results of nasal septum injury in children. Int J Pediatr Otorhinolaryngol 10:137–141, 1985.
- Levi J, McKee-Cole K, Barth P, Brody R, Reilly J. Outcomes of recalcitrant idiopathic epistaxis in children: Septoplasty as a surgical treatment. Laryngoscope. 2016;126(12):2833-2837.
- Boenisch M, Tamas H, Nolst Trenite GJ. Influence of polydioxanone foil on growing septal cartilage after surgery in an animal model: new aspects of cartilage healing and regeneration (preliminary results). Arch Facial Plast Surg. 2003 Jul-Aug;5(4):316-9.
- Menger DJ, Tabink IC, Nolst Trenite GJ. Nasal Septal Abscess in Children: Reconstruction with Autologous Cartilage Grafts on Polydioxanone Plate. Arch Otolaryngol Head Neck Surg. 2008 Aug;134(8):842-7. doi: 10.1001/archotol.134.8.842.
- Healy G, Tardy M. Septorhinoplasty in children. Operative Techniques in Otolaryngology-Head and Neck Surgery. 1994;5(1):22-26.
- Stewart MG, Witsell DL, Smith TL, Weaver EM, Yueh B, Hannley MT, Development and validation of the nasal obstruction symptom evaluation (NOSE) scale, Head Neck Surg. 130 (2004) 157–163.
- Yilmaz M, Guven M, Akidil O, Kayabasoglu G, Demir D, Mermer H. Does septoplasty improve the quality of life in children?. Int J Pediatr Otorhinolaryngol. 2014;78(8):1274-1276.
- Can İ, Ceylan K, Bayiz Ü, Ölmez A, Samim E. Acoustic rhinometry in the objective evaluation of childhood septoplasties. Int J Pediatr Otorhinolaryngol. 2005;69(4):445-448.
